
Transmural Migration of a Retained Surgical Sponge; A Case Report
Abstract
Introduction
A retained surgical towel in the abdomen is a serious postoperative complication and the most avoidable. Known as “gossypiboma”, it may migrate into adjoining cavities like the stomach, small bowel, colon, vagina, urinary bladder, pericardium, and urethra.
Case Report
A 32-year-old male presented with complaints of abdominal pain, 4 months after a laparotomy for complicated appendicitis. Initial history and presentation gave an impression of a lower urinary tract obstruction. However, symptoms progressed with signs of bowel obstruction and investigations pointed to a possible retained foreign body. This was confirmed on laparotomy with indications of a transmural migration during the period of evaluation. The report discusses the pathophysiology and manifestations of a migratory surgical gossypiboma.
Conclusions
A rare case of gossypiboma displaying transmural migration is reported. This showed an initially peritoneally placed sponge that migrated into the intestinal lumen with the sudden presentation of obstructive symptoms. Routine practice of the World Health Organization Surgical Safety Checklist can significantly prevent these incidents.
Article Information
- Received
- Accepted
- Published
Academic Editor: Anubha Bajaj, Consultant Histopathologist, A.B. Diagnostics, Delhi, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2026 Taah-Amoako Philip, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Taah-Amoako Philip, Tain District Hospital, P. O. Box 100, Nsawkaw —
Competing Interests
We declare that there is no conflict of interest.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Gossypiboma, a term of Latin origin “Gossypium” meaning cotton and the Swahili “boma” meaning place of concealment1. It refers to a surgical towel retained in the abdominal cavity after a surgical procedure. It is a serious and debilitating condition. Its incidence remains unclear as it is hardly reported due to the possible legal implications. It is however estimated to occur in 1 out of 1,000- 1,500 intra-abdominal surgeries and 1 out of 300-1,000 of all surgeries. It is totally avoidable.
The retained surgical towel may migrate into the stomach, ileum, small bowel, colon, vagina, urinary bladder, pericardium, urethra and diaphragm. They often present with bowel obstruction, bowel perforation, peritonitis, sepsis or a fistula formation2. Though extensively reported in literature, cases are still rare3, 4.
Case Report
A 32-year-old male mason, presented to the outpatient clinic of a district hospital in Ghana with a 5- day history of constant lower abdominal pain, associated with nausea. He had no episodes of vomiting and no constipation. He was managed for urinary tract infection and booked for a review in 1 week. He presented 3 days later with worsening symptoms, abdominal pain having become colicky, with associated constipation, an episode of vomiting, and loss of appetite.
Further enquiry into his past medical history revealed that he had travelled to a North African country as a prospective migrant to Europe four months earlier. He fell ill whilst there and was diagnosed of appendicitis. He had an exploratory laparotomy and appendicectomy via a midline incision and had been well until his return to Ghana when he started experiencing the above.
Clinical examination showed a young man who was not acutely ill-looking, afebrile, anicteric, not pale and was well hydrated. Heart rate was 84bpm, regular with good volume; blood pressure of 128/86mmHg; an oxygen saturation of 99% on room air and a temperature of 36.5°C. His abdomen was not distended, moved synchronously with respiration, soft on palpation, but tender in the left iliac fossa. Hernia orifices were also intact. Bowel sounds were heard but low pitched. Digital rectal examination showed an empty rectal ampulla.
An impression of an intestinal obstruction due to postoperative adhesions was made. An abdominal X-ray done showed no obvious signs of bowel dilatation but an ill-defined opacification in the area of the left lumbar region (Figure 1). An ultrasonography done showed an echogenic mass in the left iliac region measuring about 4.1cm in diameter. There was no flow on colour doppler interrogation (Figure 2). At this point a diagnosis of foreign body was queried. The patient was counselled and prepared for exploratory laparotomy.
Figure 1. Erect abdominal X-Ray showing an ill-defined opacification in the left lumbar region (arrowed).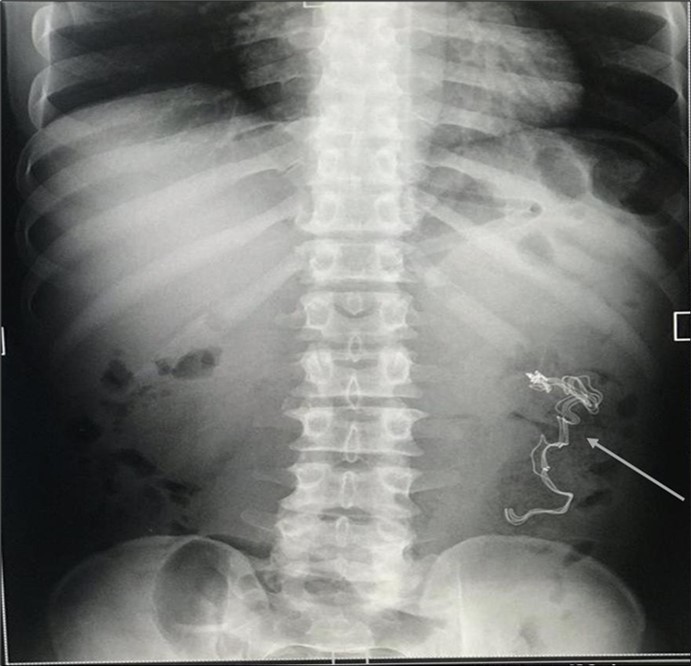
Download figure
Figure 2. Abdominopelvic USG: An echogenic mass in the left iliac region measuring about 4.1cm in diameter. There was no flow on colour doppler interrogation.
Download figure
Intraoperatively, there was no free fluid in the peritoneum, dilated loops of small bowel were noted with adherence to the left lower quadrant of the abdominal wall. Adhesions were broken down and a firm intraluminal mass, approximately 20cm in length was noticed lurking out of the site of an iatrogenic injury made in the jejunum from the adhesiolysis. This was easily milked out (Figure 3). A resection of 20cm of the jejunum was done with an end-to-end anastomosis.
Figure 3. A picture showing the intraluminal mass within the lumen of the jejunum (A) which was milked slowly out of the bowel (B). The defect in the bowel (C) is seen after the mass is completely out. The mass (D) was opened up to show its character (E), a surgical sponge.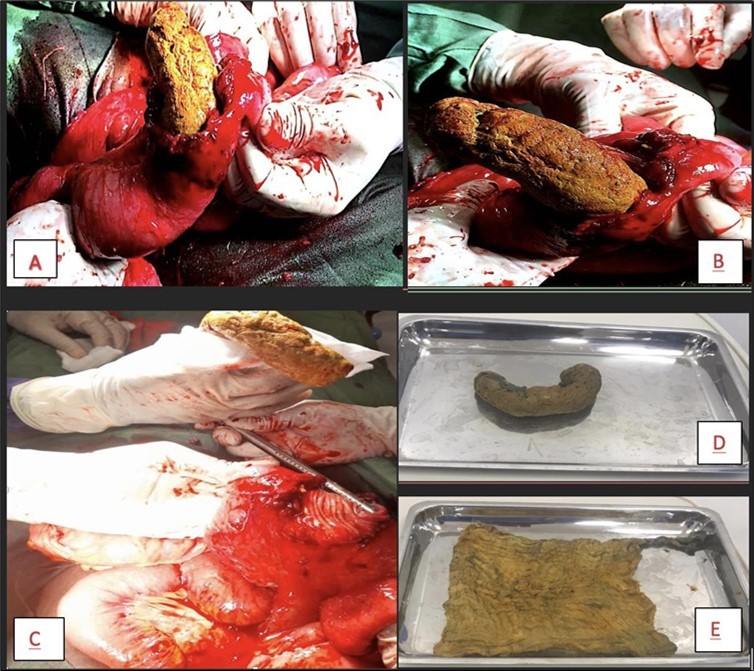
Download figure
He recovered well and was discharged home on postoperative day 7. He was seen on follow-up review 1 and 2 months after surgery and was doing well.
Discussion
Retention of gauze material in the body inadvertently, though preventable is not uncommon. Its occurrence is often unrelated to the indication for the surgery nor the surgical technique but a failure to do due diligence in adhering to basic theatre protocols by ensuring accurate instrument count and documentation. Though no body cavity is spared, it is frequently reported in the abdominal cavity like in this patient 5, 6, 7, 8.
The first case of gossypiboma was reported by Dr. Henry P. C. Wilson in 18849. The first legal suit on gossypiboma was reported in 1933 though some authors have revealed judgements on it dating as far back as 189710. Approximately 300 cases have since been reported to date in the English literature with most emanating from the developing world11. The true incidence remains unknown due to under reporting as embarrassment and medicolegal issues may emanate therefrom12.
Dakubo et al in 2013 prospectively studied the incidence in a tertiary facility in Ghana following an index case recorded in 200313. In the 10-year study, 12 cases were recorded involving 9 females and 3 males. 7 of the surgeries were performed in the tertiary facility, 2 in municipal hospitals, 2 in private hospitals and 1 in a quasi-public hospital. Of the cases conducted in the tertiary facility, estimated gossypiboma rate was 2.5 per 10,000 surgeries. 10 out of the 12 cases recorded followed intra- abdominal surgeries. The others were complications from thyroidectomy and mastectomy.
The causes of gossypiboma have been attributed to poor preparations in emergency surgeries, impromptu change in surgical procedure, sponge counts hurriedly done, inexperienced staff, poor intraoperative communication, inadequate staffing, long surgeries, obesity, complex surgeries, damage control surgeries and surgeries in more than one body cavity9, 12. According to Gawande et al, emergency surgeries have a risk ratio of 8.8 (95% CI, 2.4-31.9), unplanned change in the surgical procedure, 4.1 (95% CI, 1.4-12.4) and high body-mass index, 1.1 (95% CI, 1.0-1.2)14. The patient presented was not obese, and we could not ascertain any of the other factors as the initial surgery was conducted in a different jurisdiction.
Erosion of a surgical sponge into the gastrointestinal tract is an unusual phenomenon. This is attributed to the pressure exerted by the foreign body forcing a cavitation into the hollow organ. This was suspected in the patient presented as the initial impression on X-ray was a foreign body in the peritoneum and there were no obstructive symptoms on initial presentation. Transmural migration commonly occurs in the small intestine as its wall offers little resistance15. The least common site of migration is the stomach, due to its relatively small external surface area, its thick wall and its higher location in the abdominal cavity16.
In an experimental study, Wattanasirichaigoon placed pieces of gauze measuring (4 x 4) cm at different regions within the peritoneal cavity in Wistar rats. In 10 out of 36 animals, invasion into the intestinal lumen occurred17. There was no migration into other organs. Four stages of migration were described. The first involved a foreign body reaction, followed by secondary infection, then mass formation and finally remodelling18.
During a foreign body reaction, the omentum together with some loops of jejunum wall off the sponge, encapsulating it. With a continuous contact with the viscera, parts become ischemic and inflamed, stimulating lytic enzymes which dissolve the tissues involved. The second stage of secondary infection occurs when the cotton filament reaches the intestinal lumen and, reacting with the various intestinal enzymes with a resultant cytolysis. During the subsequent mass formation, there is a spread of infection throughout the sponge. A thick fibrous wall is formed preventing the spillage of the contents into the peritoneal cavity. Thus, a mass is formed comprising of dilated loops of jejunum or ileum with the sponge within the mass and the lumen of the mass in continuity with the lumen of the bowel. Cotton filaments are then released into the lumen. A fibrotic scar is formed after the whole surgical sponge is released into the lumen in the final stage of remodelling18.
Surgical intervention is the mainstay of treatment. With radiological diagnosis, conservative management can be considered in cases of partial or complete erosion of a retained sponge. However, only 4 cases of complete transmural migration and expulsion have been reported19.
Gossypiboma is preventable and as such preventive measures should always to practiced. Standard procedures like the use of the World Health Organisation (WHO) Surgical Safety Checklist should be adopted20. Accurate sponge count before surgery and before wound closure together with a methodical examination of the abdomen is advised. Though not universal, adoption of this simple practice can be lifesaving. Situations have, however, been recorded where falsely correct sponge counts were documented 21.
“Tagging” of surgical sponges is also advocated which will enable them to appear as hyperdense, linear structures on radiography, if retained, thus aiding in early diagnosis if suspected22.
Conclusion
We report this rare case of gossypiboma displaying transmural migration. It shows an initial peritoneally placed sponge migrating into an intestinal lumen with sudden presentation of obstructive symptoms. Routine practice of the WHO Surgical Safety Checklist and methodical inspection of the abdomen before wound closure can significantly prevent these incidents.
Declarations
Informed consent
Written informed consent was obtained from the patient for the publication of this study and any accompanying images.
References
- 1.Sözütek A, Karabuǧa T, A D Bozdaǧ, Derici H. (2010) Asymptomatic gossypiboma mimicking a liver mass,”Turk. , J Surg 26, 225-228.
- 2.A, D M Studdert, E John Orav, T A Brennan, M J Zinner et al. (2003) Risk Factors for Retained Instruments and Sponges after Surgery From the Departments of Surgery.
- 3.Zantvoord Y, Weiden R M F Van Der, Hooff M H A Van. (2008) . Number 7 OBSTETRICAL AND GYNECOLOGICAL SURVEY,” .
- 4.Erdil A. (2008) Transgastric migration of retained intraabdominal surgical sponge:. , Gossypiboma in the Bulbus,”Internal Medicine 47, 613-615.
- 5.Yamamura N. (2008) Intra-abdominal textiloma. A retained surgical sponge mimicking a gastric gastrointestinal stromal tumor: Report of a case,”Surg Today. 38, 552-554.
- 6.Burrel M, Capurro S, Arguis P, Vilana R. (2000) Sonographic Appearance of a Retained Surgical Sponge in the Neck,”.
- 7.Erdem G, Ateş Ö, Koçak A, Alkan A. (2010) Lumbar gossypiboma,”Diagnostic and Interventional Radiology. 16, 10-12.
- 8.Tan V E S, D S Sethi. (2011) Gossypiboma: An unusual intracranial complication of endoscopic sinus surgery,”Laryngoscope. 121, 879-881.
- 10.Garg M, A D.Review Paper A Review of. , Medicolegal Consequences of Gossypiboma.” J Indian Acad Forensic Med 32(4).
- 11.Asirdizer M, Karapirli M, Uysal C, Yilmaz K, Akgöz S. (2009) The medico-legal importance of gossypiboma: case report (poster presentation). [Gossipibomanın mediko-legal önemi: olgu sunumu (poster bildiri)-ENGLISH] PP-177 VVIDESPREADING PROBLEM: BULLYING,”. 10-13140.
- 12.A E Lincourt, Harrell A, Cristiano J, Sechrist C, Kercher K et al. (2007) . , Retained Foreign Bodies After Surgery,”Journal of Surgical Research 138, 170-174.
- 14.A, D M Studdert, E John Orav, T A Brennan, M J Zinner et al. (2003) Risk Factors for Retained Instruments and Sponges after Surgery From the Departments of Surgery (A,”.
- 15.R J Cruz, Figueiredo L F Poli de, L R Guerra. (2003) Intracolonic Obstruction Induced by a Retained Surgical Sponge after. , Trauma Laparotomy.”Journal of Trauma 55(5), 989-991.
- 16.B, Yilmaz E, Sen M, Kayhan B, Görgül A et al. (1997) . , Transgastric Migration of a Surgical Sponge.”J Clin Gastroenterol 24(1).
- 17.Wattanasirichaigoon S. (1996) Transmural migration of a retained surgical sponge into the intestinal lumen: an experimental study.”J Med Assoc Thai. 79(7), 415-422.
- 18.C E Fabian. (2005) Electronic tagging of surgical sponges to prevent their accidental retention.”. , Surgery 137(3), 298-301.
- 19.Zantvoord Y, Weiden R M F Van Der, Hooff M H A Van. (2008) . Number 7 OBSTETRICAL AND GYNECOLOGICAL SURVEY,” .
- 20.Liam Donaldson Weiser, Gawande Atul. (2009) WHO guidelines for safe surgery. World Health Organization.