Assessment of Syndemic Inter-relationships between Substance Use, Violence and HIV Risk Among Persons Seeking Emergency Care in Nairobi, Kenya
Abstract
Introduction
Contemporaneous substance abuse, violence and HIV/AIDS risks (SAVA) result in synergistic negative impacts (syndemic effects). Presence of and risks for syndemic SAVA conditions are common among emergency department (ED) patients, however research on these inter-related processes is limited in sub-Saharan Africa. This study utilizes structural equation modeling to examine the relationships of syndemic SAVA conditions among persons seeking emergency injury care in Nairobi, Kenya.
Methods
This secondary analysis of a prospective observational study examined SAVA syndemic conditions among non-pregnant, adult ED injury patients able to provide consent at Kenyatta National Hospital. Structural equation modeling using diagonally weighted least squares (DWLS), was used to quantify associations between three latent variables (substance use, HIV risks, violence exposure). HIV risk included partner HIV status, men who have sex with men (MSM), and gay identities; violence exposure covered emotional, physical or sexual violence in the past six months; substance use encompassed positive screening for alcohol use disorder, poly-substance use, injection drug use and injury-related substance use. Model fitness was assessed using the Bentler-Bonett Normalized Fit Index (BB NFI), Goodness of Fit Index (GFI) (>0.9) and standardized root mean square residual (SRMSR) (< 0.05). Covariance between the latent factors was estimated.
Results
Among 2,368 screened ED patients, 665 were enrolled. Males were 83% of the sample; median age was 30 years (IQR: 24-38). Fit indices using DWLS showed a close fitting model (GFI=0.99, BB NFI=0.95, SRMSR=0.04). The indicator variables had significant loadings on two of the three syndemic factors (substance use and violence exposure, β range 0.10-0.95); in the SEM only MSM status had a significant loading on HIV risk, which was insufficient to confirm the identification of the latent factor. Violence exposure and substance use risk had significant positive covariance (0.30, p<0.001).
Discussion and Conclusion
This study provides the first available data from ED patients in sub-Saharan Africa on SAVA conditions, showing a co-relationship of violence exposure and substance use but no significant associations with HIV risk. These results can be used to inform programmatic interventions for higher-risk persons addressing synergistic conditions during emergency care.
Author Contributions
Academic Editor: Shivaji Kashinath Jadhav, Orange Health Infectious Laboratory, Bangalore, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2026 J. Austin Lee, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have no competing or financial interests to disclose.
Citation:
Introduction
The SAVA syndemic is the interconnected relationship between substance abuse, violence, and HIV/AIDS, where these factors collectively exacerbate health disparities and present mutually reinforcing challenges.1, 2 This syndemic highlights how substance use increases vulnerability to both violence and HIV transmission, while violence further complicates HIV risk and treatment adherence. Alcohol and illicit drug consumption are associated with increased HIV risk through sexual behaviors, including unprotected sex, inconsistent condom use, multiple partners and sexual violence.3, 4, 5 Alcohol use and intoxication have been linked to increased violence.6, 7 Violence and HIV are interconnected public health challenges, with high levels of violence among individuals accessing HIV services; prior evidence from Kenya showed that targeted prevention and response strategies can synergistically reduce both violence and HIV risk factors.8, 9 Substance use is strongly associated with experiencing violence among sex workers and people who inject drugs (PWID) with studies highlighting its role in exacerbating HIV and broader health risks.10, 11
Prior work evaluating the SAVA syndemic has focused on women and urban settings in the United States.12, 13, 14, 15, 16, 17, 18, 19, 20, 21 Internationally, the SAVA syndemic has been investigated among populations of Hispanics22, Kazakh women23, Uganda youth,24, 25 and among both female and male populations in South Africa.26, 27, 28 Within Kenya, there is a recognition that the risk factors for the SAVA syndemic are prevalent and have been studied in focused populations, including: PWID,11 sex workers, 10, 29, 30, 31, 32 heavy alcohol users,33 and among men who have sex with men (MSM).34 These studies highlight the importance of addressing interconnected challenges in marginalized groups through interventions that target social and structural factors.17 Substance use and violence among persons seeking care in emergency care is common, and those persons also have been shown to have higher-risk profiles for contracting and transmitting HIV.35, 36, 37, 38, 39, 40, 41, 42 In sub-Saharan Africa where HIV, violence and substance use levies some of the largest burdens globally there is limited data evaluating SAVA syndemic conditions, and no extant data from emergency care populations.43, 44, 45, 46, 47 Therefore to address the gap in the evidence-base and inform understanding of SAVA syndemic conditions and potential programmatic solutions this study used advanced statistical modeling to investigate relationships between syndemic SAVA conditions among persons seeking emergency care in Kenya.
Methods
Study design and Setting
This study was a cross-sectional secondary analysis of prospective data from a continuously enrolled population of patients presenting with injuries to the Kenyatta National Hospital (KNH) ED in Nairobi, Kenya. Data was collected from March to August 2023 and derived from a study assessing HIV care delivery in this setting.48 KNH is the largest hospital in Kenya, and serves as the primary injury center for Nairobi and a national referral hub. The KNH ED provides 24-hour emergency services and has embedded HIV Testing Services freely available day and night.49, 50, 51
Selection of Participants
Patients were recruited from all individuals seeking ED care; eligible patients were adults aged 18 years or older, obtaining injury care at the KNH ED and able to provide informed consent. Exclusions included non-injury cases, incarcerated persons, pregnant individuals, and critically ill patients or those unable to consent. All enrolled participants provided informed consent, with study information and consents available in Kiswahili and English, and research staff were fluent in both languages. The study was approved by both the KNH Ethics and Research Committee and the Institutional Review Board of Rhode Island Hospital.
Data Collection and Management
Participants received standard ED care for injuries from non-study providers. Screening and consent were conducted in a private area to ensure confidentiality, with enrollment occurring as soon after triage as able. Data collected included demographics, medical history, social history injury details, interpersonal violence history, and ED care outcomes.49 All data were securely stored in electronic databases using password-protected devices accessible only to study staff.52, 53
SAVA Variables
Empirical approaches to the SAVA theory have relied on steps that require simplification of complex interactions and can fail to capture the nuanced interactions between substance abuse, violence, and HIV/AIDS.54 A prior scoping review of SAVA research revealed that the majority of studies relied on regression analyses rather than employing other methods, that could be superior in evaluating the complex inter-relationships.17
Demographic, HIV risk, substance use, and violence risk factors were utilized for modeling and analysis. Data for all variables were based on participant self report. Demographic variables included age at time of ED visit and biological sex. HIV risk factors included sexual identity (gay and/or MSM), sex partners HIV status, condom use practices during the last six months, history of injecting drug use, transactional sex (money or other goods exchanged to give or receive sex), and following the Kenya national guidelines on recommend HIV testing frequency (if age 18-24 years testing every 6 months, if age ≥25 years and no other risk factors testing every 2 years, if high risk ≥18 years testing every 3 months).55 Substance use risk factors included: illicit drug use during the last 6 months, drug use during the time of injury, history of polysubstance use, and being at risk for hazardous alcohol use based on the validated Alcohol Use Disorders Identification Test Consumption (AUDIT-C) questions (females scoring ≥3 and males ≥4).56, 57, 58 Violence exposure risk factors included report of either emotional, physical or sexual violence in the past 6 months.47, 59
Data Management & Analysis
Data was imported into SAS (Version 9.4, SAS Institute Inc, Cary, N.C.) for analysis. Descriptive statistics are reported as means with standard deviations (SD), medians with interquartile range (IQR), or percentages where appropriate. Prior to modeling, data used in the analysis were transformed into binary values (age 18-24 versus older, yes or no to substance use variables, positive or negative for AUDIT-C, HIV risk present or not, etc. Due to low frequencies for variables defining key populations including ever injecting drugs (n = 4), MSM (n = 5), gay (n = 4), and commercial sex work (n = 9) a summary composite ordinal variable was derived and used in modeling analyses for HIV risk.
Structural equation modeling (SEM) was used to identify measured indicator variables associated with three latent factors; HIV risk, violence exposure, and substance use risk. SEM is a statistical approach used to evaluate relationships between observed and latent (unobserved) variables to better understand direct and indirect effects within a system of relationships.60, 61 The SEM method has been used in a variety of other settings62, 63, 64, 65 , however, this methodology has not previously been utilized to evaluate the SAVA syndemic in emergency care settings. SEM combines factor analysis (to define the underlying latent factors from their measured manifest variables) and predictive models (assessing the covariance between the latent constructs). Model fitness was evaluated by assessing the Bentler-Bonett Normalized (BB NFI) and Goodness of Fit Indices (GFI, acceptable values >0.90) and the standardized root mean square residual (SRMSR, acceptable values <0.05). The covariance between the proposed three latent syndemic factors was also estimated.
An exploratory and confirmatory factor analysis was conducted, a random sample of 400 participant data was selected for the exploratory model, and the full sample used in the confirmatory model. As binary variables were being used in these analyses, the diagonally weighted least squares (DWLS) estimation method was used. Following the SEM analysis a mediation model was added to assess the potential mediating effect of key populations for HIV on the relationship between the identified latent risk factors.66
Results
Characteristics of study subjects
During the study period 2368 patients presenting to the KNH ED were screened for participation. Among those, 1078 (45.5%) did not meet inclusion criteria and 625 (26.4%) declined participation. A total of 665 patients were consented and enrolled (Figure 1). Males were 83% of the sample and the mean age was 32 years (standard deviation of 10.5 years). Patient characteristics regarding SAVA syndemic factors are summarized in Table 1. A number of findings suggest increased risks for syndemic SAVA conditions among enrollees, including: not knowing sexual partner(s) HIV status (89.6%), high levels of illicit drug use during the injury event that led to the ED encounter (18.5%), and high rates of prior 6-month experiences of physical violence (18.9%).
Figure 1.Patient Enrollment and SAVA Syndemic Risks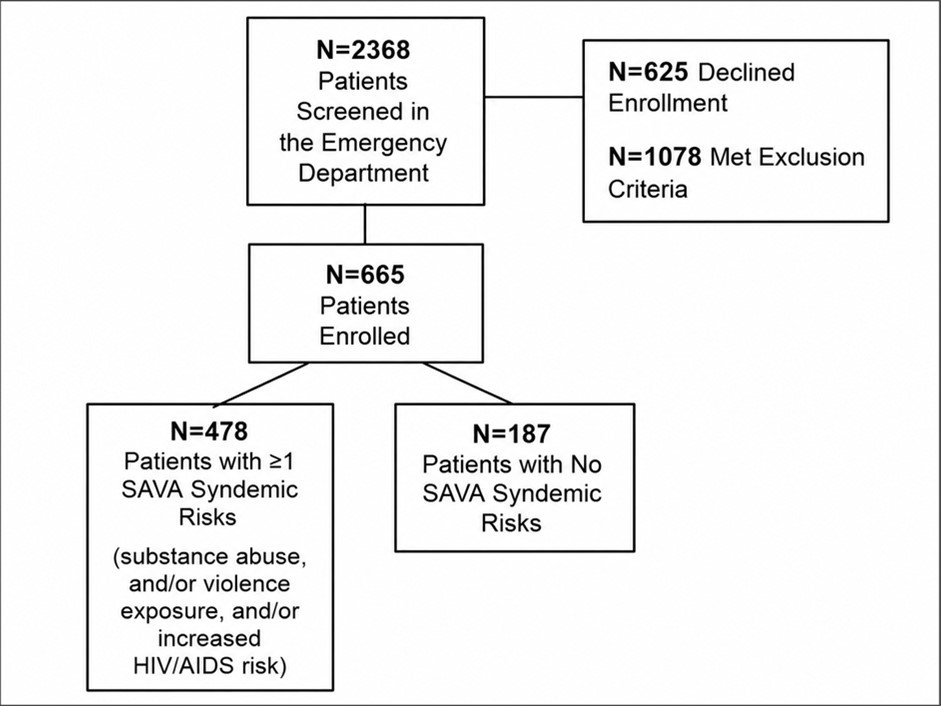
| n (%) | |
| HIV Risk | |
| Sexual Identity | |
| MSM | 5 (0.8%) |
| Gay Man | 4 (0.6%) |
| Know Sex Partner(s) HIV Status | |
| Yes | 69 (10.4%) |
| No | 596 (89.6%) |
| Past 6-months Consistent Condom Use | |
| Yes | 383 (57.6%) |
| No | 282 (42.4%) |
| Prior Injected Drug Use | |
| Yes | 4 (0.6%) |
| No | 661 (99.4%) |
| Commercial Sex Work | |
| Yes | 9 (1.5%) |
| No | 656 (98.6%) |
| HIV Testing Compliant | |
| Not tested | 83 (12.7%) |
| Tested but not compliant | 84 (12.8%) |
| Tested and compliant | 489 (74.5%) |
| Substance Use Disorder risk | |
| Past 6-months Illicit Drug Use | |
| Yes | 185 (27.8%) |
| No | 480 (72.2%) |
| Drug use During Injury Event | |
| Yes | 123 (18.5%) |
| No | 542 (81.5%) |
| History of Poly-substance Use | |
| Yes | 146 (22.0%) |
| No | 519 (78.0%) |
| At risk for Hazardous Alcohol Use: Positive Alcohol Use Disorders Identification Test–Consumption | |
| Positive | 162 (24.4%) |
| Negative | 503 (75.6%) |
| Violence Risk | |
| Past 6-months Exposure to Physical Violence | |
| Yes | 126 (18.9%) |
| No | 539 (81.1%) |
| Past 6-months Exposure to Sexual Violence | |
| Yes | 25 (3.8%) |
| No | 640 (96.2%) |
| Past 6-months Exposure to Emotional Violence | |
| Yes | 73 (11.0%) |
| No | 592 (89.0%) |
Structural Equation Modeling Results
The exploratory and confirmatory SEM yielded two identified latent constructs that were supported by the overall fit indices and beta coefficients of the individual variables on the factor (Figure 2). The overall fit indices indicated a close fitting two-factor model (GFI=0.98, BB NFI=0.95, SRMR=0.04). The indicator variables had significant loadings on two of the three syndemic variables, substance use risk and violence exposure (ranging 0.25 to 0.95), but only MSM had a significant factor loading on the putative HIV risk factor, insufficient to determine that the latent factor had been identified. Additionally, violence exposure and substance use risk had significant and positive covariance (β=0.30, p<0.001).
Figure 2.Structural Equation Model Two Factor Solution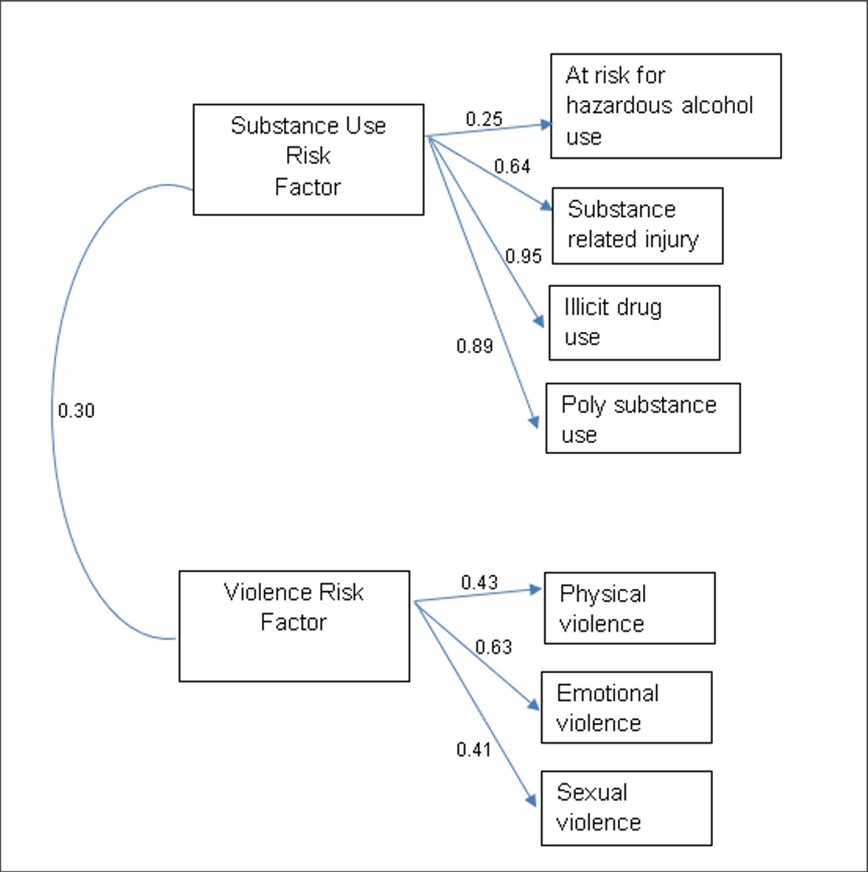
Following the SEM, a mediation path analysis was conducted with the direct path between substance use risk and violence risk compared to a mediated pathway between substance use risk and violence risk when key populations the mediating variable (Figure 3). Fit indices for this were within acceptable ranges (GFI=0.92, BB NFI=0.94, SRMR=0.05). Illustrated in Figure 3 the direct path between substance use risk is significant and positive in the direct path (c=0.24, p<0.001). The inclusion of the mediation variable, the key population composite HIV risk, partially mediated the relationship between substance use and violence. The direct path remained significant (c’=0.22, p < 0.001) and the indirect paths between substance use and key populations (a=0.15, p < 0.001) and key populations and violence risk (b = 0.08, p < 0.05) were also significant (Figure 3).
Figure 3.Mediation Model of Key Populations for HIV of Path between Substance Use Risk Factors and Violence Risk Factors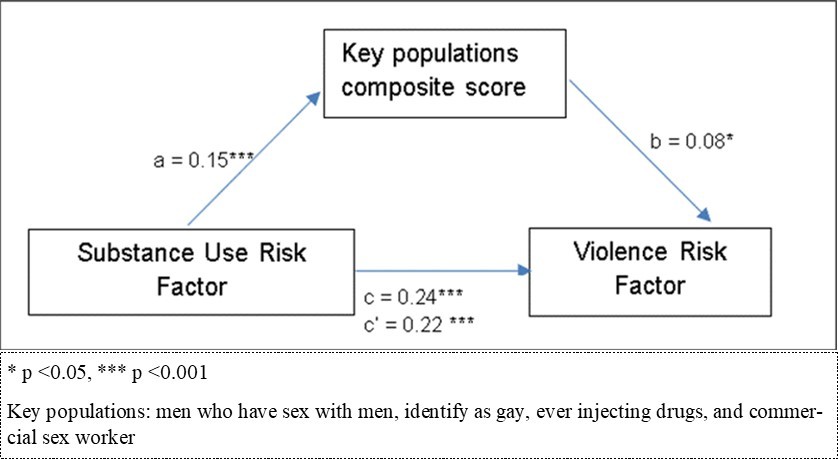
Discussion
In the current data a significant link was found between substance use and violence exposure which was mediated by the HIV risk. This advanced SEM analysis provides insight into the interplay of SAVA syndemic factors in the emergency care population from Kenya that has not been previously studied through a syndemic lens. The results can be used to inform development of programming to mitigate syndemic impacts in emergency care settings in Kenya and other similar settings. Given the nature of methods and context we propose that these findings are not a definitive framework for understanding all HIV-related SAVA relationships.
This study affirms prior research by highlighting the interplay between substance use violence, and HIV, and advances the evidence to the never before studied population of emergency care patients in Kenya, in relation to SAVA syndemic understanding.67 The high prevalence of violence, substance and HIV risk variables among the participants illustrates the potential role emergency care interactions could play in accessing persons affected by the syndemic burdens. Given the frequency of emergency care visitation in Africa, and the developing role that these care settings play in accessing and providing resources for higher-risk persons negatively affected by substance use, violence and HIV, research to leverage these interactions is needed.42, 48, 49, 68, 69, 70 There is the potential to integrate interventions amidst existing emergency care and HIV testing services, even in a context that must deal with intermittent resource limitations. Given the early stage of this field of study, understanding of effective approaches for SAVA integrated screening, brief interventions and referral to treatment (SBIRT) programs would be informative and build on the prior works that have been done in these spaces.51, 71, 72, 73, 74
Distinct from previous work the non-significant association between substance use or violence and HIV risk factors, which diverges from prior research in South Africa and Uganda where such associations were seen. 75, 76, 77 Other findings in sub-Saharan Africa have shown a correlation between violence and increased HIV risk.78 This discrepancy may be due to differences in population characteristics, or the specific indicators of HIV risk utilized in this analysis. Notably, prior studies have largely focused on women, or youth, whereas this study centers on a largely male, injured, adult group that may exhibit distinctive patterns of syndemic interaction, which are important to understand in development of person-centered programming to address syndemic impacts. As illustrated in the analysis, although the SEM did not fit all latent variables the HIV risk was found to mediate the associated path between violence and substance use suggesting that the relationship is explained via the HIV risk variable for key populations. As there is a large body of literature demonstrating key population risks for violence victimization and substance use, as well as HIV, this relationship is congruent with the extant epidemiologic data.69, 79, 80, 81 Given reaching persons from key populations is integral to achieving global HIV epidemic control the current findings highlight how comprehensive services addressing syndemic disease may be an important component for key populations in emergency care settings.
Limitations
This study represents a significant step in understanding the SAVA syndemic in an ED context, yet several considerations should be made when interpreting the findings. This sample did not capture a number of potentially contributory risk factors such as mental health conditions, economic instability, or structural inequities among the injured patients included for analysis. HIV risk factors were limited to specific and somewhat heterogeneous indicators and may not have fully captured the entire spectrum of HIV vulnerabilities, particularly among a large urban population. Additionally, measures of substance use may not fully capture substance abuse in the population, although prior work has shown that screening for substance use can serve as a proxy for substance abuse.82, 83 This study was based at a single urban ED site which may limit the ability to capture a broader set of SAVA exposures or cultural risk factors. The single site nature and study sample size limit generalizability. Future research could aim to better measure longitudinal outcomes, such as HIV treatment adherence, recurrence of violence, and substance use relapse, to better understand the syndemic's broader health impacts.
Conclusion
This study provides important insights into the synergistic challenges of substance use, HIV risk factors, and violence exposure among injured ED patients in Nairobi, Kenya. This study addressed a critical gap by focusing on an ED setting in Kenya, providing data from a high-burden, low-resource context often overlooked in the SAVA syndemic research. The analysis revealed a strong relationship between substance use and violence exposure, highlighting their mutual influence. However, the findings did not demonstrate significant associations between HIV risk factors and the other syndemic components, underscoring the complexity of these interactions within this population.
These results emphasize the need for targeted interventions during emergency care to address the intertwined issues of substance use and violence, particularly in locations where the burden of the SAVA syndemic is greatest. By leveraging advanced methodologies to better understand these dynamics, this study provides a framework for designing prevention strategies that address the root causes and overlapping impacts of these conditions in high-risk populations.
Declarations
Funding
ARA and the overall work was supported by the National Institute of Allergy and Infectious Diseases (grant number: K23AI145411). Disclaimer: The contents of this manuscript are solely the responsibility of the authors and do not necessarily represent the official views of affiliated institutions or funding bodies.
Ethics approval
The study was approved by both the Kenyatta National Hospital (Nairobi, Kenya) Ethics and Research Committee and the Institutional Review Board of Rhode Island Hospital (Providence, RI, USA).
Consent
All participants provided informed consent, with study information and consents available in Kiswahili and English
Data, Materials and/or Code availability
The data that support the findings of this study are available from the corresponding author, JAL, upon reasonable request.
References
- 1.Singer M. (2006) A dose of drugs, a touch of violence, a case of AIDS, Part 2: Further conceptualizing the Sava Syndemic. Free Inq Creat Sociol. 34, 39-54.
- 2.Gilbert L, Raj A, Hien D, Stockman J, Terlikbayeva A et al. (1999) Targeting the SAVA (Substance Abuse, Violence, and AIDS) Syndemic Among Women and Girls: A Global Review of Epidemiology and Integrated Interventions. J Acquir Immune Defic Syndr. 69-2.
- 3.Kalichman S C, Simbayi L C, Vermaak R, Jooste S, Cain D. (2008) HIV/AIDS risks among men and women who drink at informal alcohol serving establishments (Shebeens) in Cape Town, South Africa. Prev Sci Off J Soc Prev Res. 9, 55-62.
- 4.TGM Sandfort, Knox J R, Alcala C, El-Bassel N, Kuo I et al. (1999) Substance Use and HIV Risk Among Men Who Have Sex With Men in Africa: A Systematic Review. J Acquir Immune Defic Syndr. 76-34.
- 5.Kagee A. (2023) Substance use and HIV: some considerations in a global context. AIDS Care. 35, 261-4.
- 7.Klostermann K C, Fals-Stewart W. (2006) Intimate partner violence and alcohol use: Exploring the role of drinking in partner violence and its implications for intervention. Aggress Violent Behav. , Netherlands: 11, 587-97.
- 8.Artz L, Klazinga L, Müller A. (2020) Sexual and gender-based violence and HIV in South Africa: An HIV facility-based study. South Afr Med J Suid-Afr Tydskr Vir Geneeskd. 110-377.
- 9.Annor F B, Chiang L F, Oluoch P R, Mang’oli V, Mogaka M et al. (2022) Changes in prevalence of violence and risk factors for violence and HIV among children and young people in Kenya: a comparison of the 2010 and 2019 Kenya Violence Against Children and Youth Surveys. Lancet Glob Health. 10-124.
- 10.Bazzi A R, Yotebieng K, Otticha S, Rota G, Agot K et al. (2019) PrEP and the syndemic of substance use, violence, and HIV among female and male sex workers: a qualitative study in Kisumu. , Kenya. J Int AIDS Soc 22-25266.
- 11.SWKH Aung, Kingston H, Mbogo L W, Sambai B, Monroe-Wise A et al. (2023) Prevalence and correlates of violence among sexual and injecting partners of people who inject drugs living with HIV in Kenya: a cross-sectional study. Harm Reduct. 20-164.
- 12.Illangasekare S, Burke J, Chander G, Gielen A. (2013) The syndemic effects of intimate partner violence, HIV/AIDS, and substance abuse on depression among low-income urban women. , J Urban Health Bull N Y Acad Med 90, 934-47.
- 13.Illangasekare S L, Burke J G, Chander G, Gielen A C. (2014) Depression and social support among women living with the substance abuse, violence, and HIV/AIDS syndemic: a qualitative exploration. Womens Health Issues Off Publ Jacobs Inst Womens Health. 24, 551-7.
- 14.Meyer J P, Springer S A, Altice F L. (2002) Substance abuse, violence, and HIV in women: a literature review of the syndemic. , J Womens Health 20, 991-1006.
- 15.Jones A A, Gerke T, Striley C W, Osborne V, Whitehead N et al. (2019) A Longitudinal Analysis of the Substance Abuse, Violence, and HIV/AIDS (SAVA) Syndemic among Women in the Criminal Justice System. J Psychoactive Drugs. 51, 58-67.
- 16.Simon L, Livingston A, Tiamiyu K, Beals D, Muehlenhaupt A et al. (2024) . Finding the Invisible Patient to Address Substance Use, Violence, and Depression in Women Living with HIV. J CME 13, 2396256-10.
- 17.Mendenhall E, Singer M. (2020) What constitutes a syndemic? Methods, contexts, and framing from 2019. Curr Opin HIV AIDS. 15, 213-7.
- 18.Caiola C, McCoy T P, Kneipp S M. (2021) Modeling upstream socioeconomic inequities and syndemic conditions among mothers over time. Public Health Nurs. , Boston Mass 38, 186-96.
- 19.Tsuyuki K, Pitpitan E V, Levi-Minzi M A, Urada L A, Kurtz S P et al. (2017) Substance Use Disorders, Violence, Mental Health, and HIV: Differentiating a Syndemic Factor by Gender and Sexuality.AIDS Behav. 21, 2270-82.
- 20.Vavala G, Wang Q, Jimenez S, Ramos W E, Ocasio M A et al. (2022) Substance Use, Violence, and Sexual Risk Among Young Cis-Gender Women Placed at High-Risk for Human Immunodeficiency Virus Infection. AIDS Behav. 26, 3008-15.
- 21.Bulled N. (2022) A new approach to measuring the synergy in a syndemic: Revisiting the SAVA syndemic among urban MSM in the United States. Glob Public Health. 17, 2070-80.
- 22.González-Guarda R M, Florom-Smith A L, Thomas T. (2011) A syndemic model of substance abuse, intimate partner violence, HIV infection, and mental health among Hispanics. Public Health Nurs. , Boston Mass 28-366.
- 23.Jiwatram-Negrón T, Michalopoulos L M, El-Bassel N. (2018) The syndemic effect of injection drug use, intimate partner violence, and HIV on mental health among drug-involved women in Kazakhstan. Glob Soc Welf Res Policy Pract. 5, 71-81.
- 24.Logie C H, Okumu M, Malama K, Mwima S, Hakiza R et al. (2022) Examining the substance use, violence, and HIV and AIDS (SAVA) syndemic among urban refugee youth in Kampala, Uganda: cross-sectional survey findings. BMJ Glob Health. 7-006583.
- 25.Swahn M H, Culbreth R, Masyn K E, Salazar L F, Wagman J et al. (2021) The Intersection of Alcohol Use. Gender Based Violence and HIV: Empirical Findings among Disadvantaged Service-Seeking Youth in Kampala, Uganda. AIDS Behav 25, 3106-14.
- 26.Sileo K M, Sparks C S, Luttinen R. (2023) Spatial Analysis of the Alcohol, Intimate Partner Violence. and HIV Syndemic Among Women in South Africa. AIDS Behav 27-1339.
- 27.Russell B S, Eaton L A, Petersen-Williams P. (2013) Intersecting epidemics among pregnant women: alcohol use, interpersonal violence, and HIV infection in South Africa. Curr HIV/AIDS Rep. 10, 103-10.
- 28.Hatcher A M, Gibbs A, McBride R-S, Rebombo D, Khumalo M et al. (1982) Gendered syndemic of intimate partner violence, alcohol misuse, and HIV risk among peri-urban,heterosexual men in South Africa. Soc Sci Med. 295-112637.
- 29.Tegang S P, Abdallah S, Emukule G, Luchters S, Kingola N et al.Concurrent sexual and substance-use risk behaviours among female sex workers in Kenya’s Coast Province: findings from a behavioural monitoring survey. , SAHARA J J Soc Asp HIVAIDS Res Alliance 2010, 10-6.
- 30.Wilson K S, Deya R, Masese L, Simoni J M, Stoep A V et al.Prevalence and correlates of intimate partner violence in HIV-positive women engaged in transactional sex in. , Mombasa, Kenya, Int J STD AIDS 2016, 1194-203.
- 31.Roberts S T, Flaherty B P, Deya R, Masese L, Ngina J et al. (2018) . Patterns of Gender-Based Violence and Associations with Mental Health and HIV Risk Behavior Among Female Sex Workers in Mombasa, Kenya: A Latent Class Analysis. AIDS Behav 22-3273.
- 32.Poxon A, Leis M, McDermott M, Kariri A, Kaul R et al.Emergency departments as under-utilized venues to provide HIV prevention services to female sex workers in Nairobi. , Kenya. Int J Emerg Med 2023, 10-1186.
- 33.Muturi N. (2015) Gender and HIV infection in the context of alcoholism in Kenya. , Afr J AIDS Res AJAR 14, 57-65.
- 34.Kunzweiler C P, Bailey R C, Okall D O, Graham S M, Mehta S D et al. (2018) Depressive Symptoms, Alcohol and Drug Use, and Physical and Sexual Abuse Among Men Who Have Sex with Men in Kisumu, Kenya: The Anza Mapema Study. AIDS Behav. 22-1517.
- 35.McDonald A, Duncan N D, Mitchell D I. (1999) Alcohol, cannabis and cocaine usage in patients with trauma injuries. , West Indian Med J 48.
- 36.Nilsen P, Baird J, Mello M J, Nirenberg T, Woolard R et al. (2008) A systematic review of emergency care brief alcohol interventions for injury patients. J Subst Abuse Treat. 35, 184-201.
- 37.Dwommoh R, Sorsdahl K, Myers B, Asante K P, Naledi T et al. (2018) Brief interventions to address substance use among patients presenting to emergency departments in resource poor settings: a cost-effectiveness analysis. Cost Eff Resour Alloc CE. 16-24.
- 38.Forson P K, Oduro G, Bonney J, Cobbold S, Sarfo-Frimpong J et al. (2020) Emergency department admissions Kumasi, Ghana: Prevalence of alcohol and substance use, and associated trauma. J Addict Dis. 38, 520-8.
- 39.Bernstein E, Edwards E, Dorfman D, Heeren T, Bliss C et al. (2009) Screening and brief intervention to reduce marijuana use among youth and young adults in a pediatric emergency department. Acad Emerg Med Off J Soc Acad Emerg Med. 16, 1174-85.
- 40.Longo M C, Hunter C E, Lokan R J, White J M, White M A. (2000) The prevalence of alcohol, cannabinoids, benzodiazepines and stimulants amongst injured drivers and their role in driver culpability: part ii: the relationship between drug prevalence and drug concentration, and driver culpability. Accid Anal Prev. 32, 623-32.
- 41.Botchey I M, Hung Y W, Bachani A M, Paruk F, Mehmood A et al. (2017) Epidemiology and outcomes of injuries in Kenya: A multisite surveillance study. Surgery. 162-45.
- 42.Hansoti B, Stead D, Parrish A, Reynolds S J, Redd A D et al. (2018) HIV testing in a South African Emergency Department: A missed opportunity. PLOS ONE. Public Library of Science; 13-0193858.
- 43.Chen Y, Li A-D, Yang Y, Lu J, Xu Y et al. (1990) regional and national burden of HIV/AIDS among individuals aged 15-79 from. 22-51.
- 44.Igbokwe K, Onobun D E, Ononye R, Orji C, Ojo E O. (2021) Comparative Assessment of the Burden of Injury in Sub-Saharan Africa: An Analysis of Estimates From Global Burden of Disease. 16-73838.
- 45.Bajunirwe F, Maling S, Adami H-O, Ajayi I O, Volmink J et al. (2018) Burden of depressive symptoms and non-alcohol substance abuse; and their association with alcohol use and partner violence: a cross-sectional study in four sub-Saharan Africa countries. Glob Ment Health Camb Engl. 5-31.
- 46.Kenya Adolescent (2019) Mental Health Group. Burden and risk factors of mental and substance use disorders among adolescents and young adults in Kenya: results from the Global Burden of Disease Study. 67-102328.
- 47.Mercy J A, Hillis S D, Butchart A, Bellis M A, Ward C L et al. (2025) Interpersonal Violence: Global Impact and Paths to Prevention. In:. Inj Prev Environ Health [Internet]. 3rd ed. Washington (DC): The International Bank for Reconstruction and Development / Mock CN, Nugent R, Kobusingye O, Smith KR, editors .
- 48.Aluisio A R, Smith-Sreen J, Offorjebe A, Maina W, Pirirei S et al. (2024) Assessment of the HIV Enhanced Access Testing in the Emergency Department (HEATED) program in Nairobi, Kenya: a quasi-experimental prospective study. HIV Res Clin Pract. 25, 2403958-10.
- 49.Lee J A, Momanyi N, Offorjebe O A, Ngila B, Maina W et al. (2013) Characteristics of Interpersonal Violence and Intimate Partner Violence Among Injured Adults Seeking Emergency Care in Nairobi. , Kenya. R I Med J 2024, 39-45.
- 50.Aluisio A, Sugut J, Kinuthia J, Farquhar C, Mello M. (2021) Assessment of HIV testing services for patients presenting for emergency injury care in Nairobi, Kenya demonstrates beneficial potential for enhanced HIV care engagement. HIV Med. 22-246.
- 51.Lee J A, Ochola E O, Sugut J, Ngila B, Ojuka D K et al. (2022) Assessment of substance use among injured persons seeking emergency care in Nairobi, Kenya. Afr J Emerg Med. 12, 321-6.
- 52.Harris P A, Taylor R, Thielke R, Payne J, Gonzalez N et al. (2009) Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 42, 377-81.
- 53.Harris P A, Taylor R, Minor B L, Elliott V, Fernandez M et al. (2019) The REDCap consortium: Building an international community of software platform partners. , J Biomed Inform 95, 103208-10.
- 54.Chavez J V, Wang P, Larson M E, Vazquez V, M De La Rosa et al. (2023) Methodologies used in studies examining substance abuse, violence and HIV/AIDS (SAVA) constructs using a syndemic framework: a scoping review. AIDS Care. 35, 1708-15.
- 55. (2022) . National AIDS & STI Control Program (NASCOP), Ministry of Health, Kenya. Kenya HIV Prevention and Treatment Guidelines .
- 56.Vitesnikova J, Dinh M, Leonard E, Boufous S, Conigrave K. (2014) Use of AUDIT-C as a tool to identify hazardous alcohol consumption in admitted trauma patients. Injury. 45, 1440-4.
- 57.Frank D, DeBenedetti A F, Volk R J, Williams E C, Kivlahan D R et al. (2008) Effectiveness of the AUDIT-C as a Screening Test for Alcohol Misuse in Three Race/Ethnic Groups. , J Gen Intern Med 23, 781-7.
- 58.Rodríguez-Martos A, Santamariña E. (2007) Does the short form of the Alcohol Use Disorders Identification Test (AUDIT-C) work at a trauma emergency department? Subst Use Misuse. 42, 923-32.
- 60.Tarka P. (2018) An overview of structural equation modeling: its beginnings, historical development, usefulness and controversies in the social sciences. Qual Quant. 52, 313-54.
- 61.Ullman J B. (2006) Structural equation modeling: reviewing the basics and moving forward. J Pers Assess. 87, 35-50.
- 62.Yang Y. (2023) Using a Syndemic Framework and Structural Equation Modeling to Assess the Co-occurrence and Mutual Impact of Violence Experiences and Substance Use Behaviors Among Adolescents. J Interpers Violence. 38, 11595-616.
- 63.Willie T C, Kershaw T S, Blackstock O, Galvao R W, Safon C B et al. (2021) Racial and ethnic differences in women’s HIV risk and attitudes towards pre-exposure prophylaxis (PrEP) in the context of the substance use, violence, and depression syndemic. AIDS Care. 33, 219-28.
- 64.Orindi B O, Ziraba A, Bruyneel L, Floyd S, Lesaffre E. (2021) Invariance of the WHO violence against women instrument among Kenyan adolescent girls and young women: Bayesian psychometric modeling. PloS One. 16-0258651.
- 65.Luseno W K, Field S H, Iritani B J, Odongo F S, Kwaro D et al. (2021) Pathways to Depression and Poor Quality of Life Among Adolescents. in Western Kenya: Role of Anticipated HIV Stigma, HIV Risk Perception, and Sexual Behaviors. AIDS Behav 25, 1423-37.
- 66.MacKinnon D P, Fairchild A J, Fritz M S. (2007) Mediation analysis. , Annu Rev Psychol 58, 593-614.
- 67.Baral S, Logie C H, Grosso A, Wirtz A L, Beyrer C. (2013) Modified social ecological model: a tool to guide the assessment of the risks and risk contexts of HIV epidemics. BMC Public Health. 13-482.
- 68.Obermeyer Z, Abujaber S, Makar M, Stoll S, Kayden S R et al. (2015) Emergency care in 59 low- and middle-income countries: a systematic review. Bull World Health Organ. 93, 577-586.
- 69.Smith-Sreen J, Bosire R, Farquhar C, Katz D A, Kimani J et al. (2023) Leveraging emergency care to reach key populations for “the last mile” in HIV programming: a waiting opportunity. AIDS Lond Engl. 37, 2421-4.
- 70.Waxman M J, Kimaiyo S, Ongaro N, Wools-Kaloustian K K, Flanigan T P et al. (2007) Initial outcomes of an emergency department rapid HIV testing program in western Kenya. AIDS Patient Care STDs. 21, 981-6.
- 71.Westhuizen C van der, Malan M, Naledi T, Roelofse M, Myers B et al. (2021) Patient outcomes and experience of a task-shared screening and brief intervention service for problem substance use in South African emergency centres: a mixed methods study. Addict Sci Clin Pract. 16, 10-1186.
- 72.Aluisio A R, Bergam S J, Kinuthia J, Maina J W, Pirirei S et al. (2025) HIV testing services and HIV self-testing programming within emergency care in Kenya: a qualitative study of healthcare personnel to inform enhanced service delivery approaches. AIDS Care. 37, 112-23.
- 73.Fawole O I, Balogun B O, Adejimi A A, Akinsola O J, Van Wyk JM. (2019) Training medical students: victim’s perceptions of selectively screening women for intimate partner violence in health care settings. BMC Med Educ. 19-196.
- 74.O’Doherty L, Hegarty K, Ramsay J, Davidson L L, Feder G et al. (2015) Screening women for intimate partner violence in healthcare settings. Cochrane Database Syst Rev. 2015-007007.
- 75.Jewkes R K, Dunkle K, Nduna M, Shai N. (2010) Intimate partner violence, relationship power inequity, and incidence of HIV infection in young women in South Africa: a cohort study. Lancet Lond Engl. 376-41.
- 76.Geibel S, Tun W, Tapsoba P, Kellerman S. (1974) HIV vulnerability of men who have sex with men in developing countries: Horizons studies, 2001-2008. Public Health Rep Wash DC. 125-316.
- 77.Okal J, Luchters S, Geibel S, Chersich M F, Lango D et al. (2009) Social context, sexual risk perceptions and stigma: HIV vulnerability among male sex workers in Mombasa, Kenya. Cult Health Sex. 11, 811-26.
- 78.Dunkle K L, Jewkes R K, Brown H C, Gray G E, McIntryre J A et al. (2004) Gender-based violence, relationship power, and risk of HIV infection in women attending antenatal clinics in South Africa. Lancet Lond Engl. 363-1415.
- 79.Iheanacho T, Maciejewski K R, Ogudebe F, Chumo F, Slade T et al. (2022) Prevalence and correlates of depression and substance use disorders in emergency department populations: A cross-sectional study at East Africa’s largest public hospital. Afr J Emerg Med Rev Afr Med Urgence. 12, 307-14.
- 80.Batchelder A W, Foley J D, Wirtz M R, Mayer K, O’Cleirigh C. (2021) Substance Use Stigma, Avoidance Coping, and Missed HIV Appointments Among MSM Who Use Substances. AIDS Behav. 25, 1454-63.
- 81.Bain L E, Nkoke C, JJN Noubiap. (2017) UNAIDS 90-90-90 targets to end the AIDS epidemic by 2020 are not realistic: comment on “Can the UNAIDS 90-90-90 target be achieved? A systematic analysis of national HIV treatment cascades.” BMJ Glob Health. 2-000227.